Obstetric imaging
5D heart, smart imaging for screening ?
Screening for congenital heart defects by 2D ultrasound has a relatively low sensitivity, around 15-39%, which has not improved over the years despite technological improvements. However, screening for congenital heart disease is essential, as it is associated with improved pre-operative conditions, neurological outcomes and post-surgery survival(1). This is mainly due to the lack of training of operators(2,3).
Currently, the screening of congenital heart defects is based mainly on the interpretation of so-called reference cuts. The number of recommended cuts varies by country(1.4). In France, the CNEOF recommends in the 2th quarter: a "four cavities" cut, a left ejection path cut and a "3 vessels" type cut with a view of the pulmonary arterial junction(5).
The use of the volumic mode by the 3-dimensional, 10-second acquisition of the heart, called STIC (Spatiotemporal Image Correlation), was proposed more than 10 years for the study of fetal heart(6). The drawings obtained are compiled by the machine to reconstruct the volume and its movement by synchronizing them.
Thus, obtaining a volume of the heart allows, in theory, to obtain the set of cutting plans usually recommended for the examination of the fetal heart.
However, obtaining the different standard cutting plans from a single volume was reserved for expert practice, since it required a thorough knowledge of the anatomy heart and 3D(7) volume handling. Its use was therefore limited to diagnosis, for a primarily educational purpose, and not to screening.
Recently, new methods of semi-automated fetal heart examination have been proposed, such as the Fetal Intelligent Navigation Echocardiography (FINE) method. This allows to automatically generate 9 reference cuts for fetal echocardiography screening from a single ICS, and thus could be applied to the screening of congenital heart disease(8).
The hypothesis
The screening ultrasound requires a theoretical knowledge of the reference cuts, a simple manipulation of the ultrasound probe and finally a correct analysis of these cuts (quality criteria, usual aspect or not). Among these prerequisites, learning how to manipulate the probe to obtain the reference cuts appears to be one of the first difficulties encountered by the "novice" ultrasonist. Once the reference cut has been obtained, a second difficulty lies in the first stage of the interpretation of checking the quality criteria of the cut obtained before interpreting it.
The examination of the fetal heart follows a sequential approach during which the ultrasound designer will follow a process, most often not systematized, to obtain the recommended reference cuts and analyze them. This approach therefore has several limitations. The presentation of the fetal heart to the ultrasound designer may vary, depending on the fetal position, which may hinder systematization of the analysis and the achievement of good quality cuts(9,10). This sequential approach can make it difficult to obtain all the cuts required for the examination of the heart.
On the other hand, the acquisition of an STIC (dynamic volume), ranging from the stomach to supra-aortic trunks, allows in about ten seconds to obtain all the cutting plans necessary for the examination of the heart. However, "manual" navigation in this volume requires a fine knowledge of fetal cardiac anatomy and volumic manipulation, known as post-treatment.
The FINE (Fetal Intelligent Navigation Echocardiography) or 5D Heart method corresponds to "intelligent" navigation in the volume without having to perform a long and difficult post-treatment(8). Once the ICTS is obtained, positioning anatomical markers on pre-selected pairs by the software allows to model an anatomical reconstruction of the heart (Figure 1). Then, the system automatically navigates through the volume, finds and retrieves the planes, and then displays the 9 datum planes, the spine at 6 o'clock.
The possibility of obtaining a systematic and simultaneous examination of the fetal heart would therefore, in theory, allow for easier analysis, and above all a better reproducibility of the examinations.
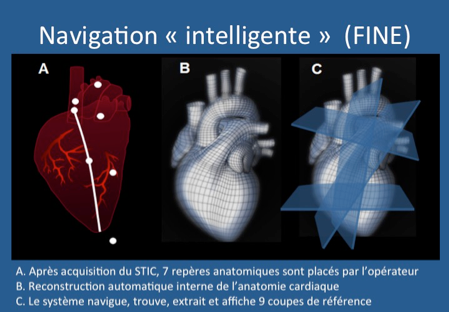
Figure 1: Stages of volumic reconstruction of the fetal heart by the FINE method (Fetal Intelligent Navigation Echocardiography).
Smart Navigation (FINE)
A. After the acquisition of the ICTS, 7 anatomical markers are placed by the
operator
B. Automatic internal reconstruction of cardiac anatomy
C. The system navigates, finds, extracts and displays 9 reference cuts
Prerequisites
In making an ICT, the quality of the cuts no longer depends on the operator for all the cuts, but only on the quality of the acquisition of the ICT.
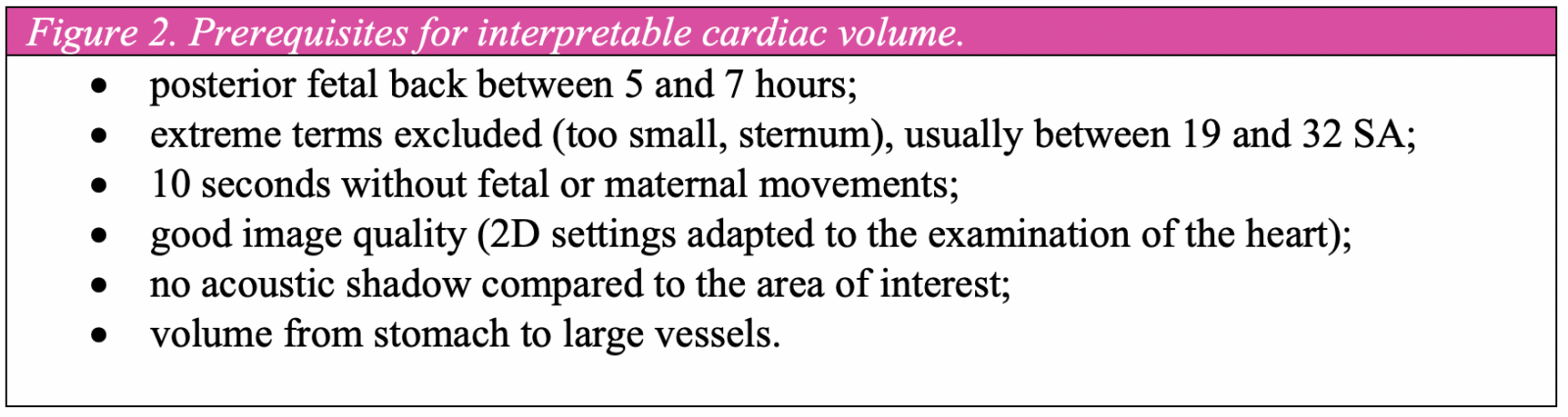
Thus, the precondition for this method is the acquisition of an ICT of the best possible quality. These criteria are summarized in Figure 2.
In practice
In practice, the ultrasonist compels himself during the examination to obtain a fetal position with a posterior back, between 5 and 7 hours in the image. By quickly translating with the sensor from the bottom to the top, from the stomach to the supra-aortic trunks, the ultrasonist verifies that the entire volume of interest can be recorded with good quality, for example by checking the absence of a member’s interposition with respect to the area of interest. Once the fetal movements have stabilized, the ultrasonist starts the acquisition from a cut four cavities, while asking the patient to hold her breathing for ten seconds. The angle of acquisition varies according to gestational age, usually more than 5° in relation to gestational age (25 to 40°). The duration of the entire process is less than 5 minutes (Video 1).
Video 1: 5D Heart Process (Samsung Co): Acquisition of ICS, application of the FINE method.
• Once the acquisition has been made, an axial-cut ciné-loop sequence is displayed to verify that the acquisition is complete and that it meets the criteria of qualifications set out in Figure 2. This list of quality criteria is displayed on the screen next to the movie-loop.
• Then, the software asks the ultrasound designer to place a cross in the center of the abdominal aorta on an abdominal axial cut. After positioning the coordinate system, a sagittal cross section of the aorta is displayed to check the absence of fetal movements (the aorta is straight on the image).
• Then, the software proposes to place markers on 7 anatomical structures (1 to 7) from 4 automatically generated axial cuts (Figure 3).
- an abdominal cut with the stomach visualization: aorta identification (1);
- a cup of the 4 caves: locating the aorta (2), the cross of the heart (3), positioning the axis of the interventricular septum (4);
- a cut of the 3 ships: identification of the pulmonary valve (5), the upper vena cave (6);
- a cut of the horizontal part of the aorta: identification of the middle of the horizontal aorta (7).
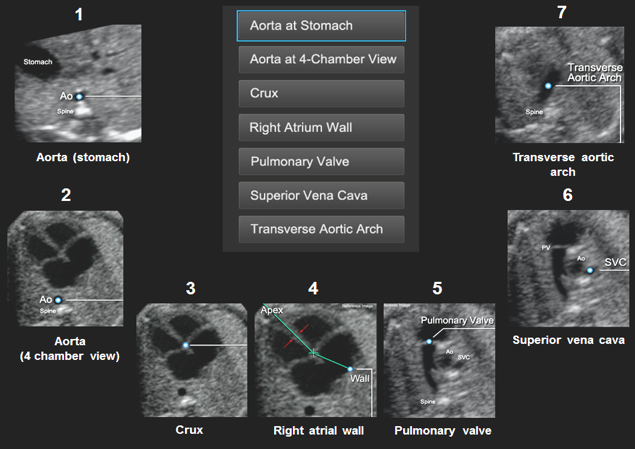
Figure 3: Positioning of the 7 anatomical markers on the 4 cuts automatically displayed by the FINE method (according to Yeo et al.).
• The system models a "personalized" anatomy of the fetal heart and generates 9 standardized cuts displayed on a single screen (video 2):
- 3 vessels,
- 4 caves,
- 5 cavities,
- departure of the aorta,
- short axis of large vessels, pulmonary junction,
- abdomen, stomach position,
- arterial canal butt,
- aorta lacrosse,
- two-cellar.
Video 2: Standardized display of the 9 reference cardiac cuts after the FINE method (according to Yeo et al.).
• Finally, if one of the cuts is not considered satisfactory, a tool allows to select a better image (Virtual Intelligent Sonographer Assistance) (Video 3).
Video 3: Using the VIS-Assist tool to select another image for the reference cut.
Smart Alerts
During this process, the positioning of the calipers can lead to the display of automatic alerts:
- alert position in the seat: the positioning of the calipers is in favor of a presentation of the seat, which allows the operator to ask the question of the situs. The images are then reversed as if for a cephalic presentation;
- alert spine movement: when the spine moves from right to left in the volume. The positioning of anatomical markers is made more difficult, thus creating less interpretable plans on the 9 sections displayed (video 4);
- alert position of the spine: when the spine is not positioned between 5 and 7 hours, the system recommends that the ICTS not be used. The operator is then informed of the possible consequences: poor visualization of the pulmonary valve, position of the upper cave vein and horizontal aorta difficult to spot and therefore not visible on the 9 cups generated (video 4).
Video 4: Display of fetal back position alert.
Use
As with any new method of examination, a learning curve is required for the completion of an ICT and the use of the FINE method(7,11). Recently, Garcia et al. showed that FINE was feasible in 72.5% (150/2007) of cases(12). In the other cases, half of no ICS had been achieved due to a spine position not between 5 and 7 h and the other half had an unsatisfactory quality of ICS (obesity). Once the film-loop was considered satisfactory, the 9 standard cuts could be obtained in 98-100% of the cases.
It is difficult to compare these results with those of the 2D ultrasound, which remains poorly evaluated. De Vore et al. showed in a study of 709 patients in the 2nd quarter screening ultrasound that four cavities were not obtained in 9.3% of cases by experienced ultrasonists(13). Tegnander et al., in a study of 29,035 ultrasound scans in the 2th quarter, showed that 4-cavities and ejections were only obtained in 75% of cases by experienced ultrasonists (> 2,000 exams per year) and 36% of cases by choéless experienced designers(14). Finally, Jaudi et al., in a randomized study that included 5,160 images on the evaluation of the quality of the four-cavities cut, reported a rate of images considered inadequate between 16 and 36%(15).
Thus, the FINE method has several advantages:
- systematize the examination of the fetal heart with strict requirements in terms of image quality;
- systematize the display of the cuts allowing easier reading;
- allow the simultaneous display of the different cuts;
- enable telemedicine.
Another benefit, essential for screening, is the process of positioning calipers. Indeed, the hypothesis for the modeling of the heart is that of a heart without malformation. If ICTS quality criteria have been met, the impossibility of placing anatomical benchmarks already corresponds to a positive screening situation before even reading the standardized cuts. For example, the inability to locate the pulmonary valve may cause a suspected pulmonary atrisy.
However, this method also has a few limitations:
- the need to have a 3D probe and know how to realize an ICTS,
- the need for optimal conditions of examination (weight, term, positioning of the fetus),
- the impossibility of making measurements on the cuts displayed.
Currently, a multi-center FINETWORK study is being conducted by Wayne State University in Detroit to evaluate the diagnostic performance of this tool.
Conclusion
The performance of ultrasound screening for congenital heart disease remains low, mainly influenced by the high variability among observers. As with the measurement of nucal clarity in the first quarter, improved screening must necessarily require better systematization of examinations(16). Now 4D ultrasound, combined with automation tools such as the FINE method, allows this systemization. For a long time limited to an expert practice for fetal heart examination, its use could be used for screening. However, the feasibility and diagnostic performance of these new semi-automated methods have yet to be demonstrated.
References
Click on the references and access the Abstracts on

1. Donofrio MT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A, et al. Diagnosis and Treatment of Fetal Cardiac Disease: A Scientific Statement From the American Heart Association. Circulation 2014 ; 129 : 2183-242. Search the abstract2. Khoshnood B, Lelong N, Houyel L, Thieulin A-C, Jouannic J-M, Magnier S, et al. Prevalence, timing of diagnosis and mortality of newborns with congenital heart defects: a population-based study. Heart 2012 ; 98 : 1667-73. Search the abstract3. Pinto NM, Keenan HT, Minich LL, Puchalski MD, Heywood M, Botto LD. Barriers to prenatal detection of congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2012 ; 40 : 418-25. Search the abstract4. Carvalho J, Allan L, Chaoui R, Copel J, DeVore G, Hecher K et al. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart: ISUOG Guidelines. Ultrasound Obstet Gynecol 2013 ; 41 : 348-59. Search the abstract5. Viossat P, Dommergues M, Lansac J. Rapport de la conférence nationale de l’échographie obstétricale et fœtale (CNEOF) – recommandations pour l’échographie focalisée. Gynécol Obstét Fertil 2015 ; 43 : 469-71. Search the abstract6. DeVore GR, Falkensammer P, Sklansky MS, Platt LD. Spatio-temporal image correlation (STIC): new technology for evaluation of the fetal heart. Ultrasound Obstet Gynecol 2003 ; 22 : 380-7. Search the abstract7. Yeo L, Romero R. How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart. J Ultrasound Med 2016 ; 35 : 1021-42. Search the abstract8. Yeo L, Romero R. Fetal Intelligent Navigation Echocardiography (FINE): a novel method for rapid, simple, and automatic examination of the fetal heart: Fetal intelligent navigation echocardiography (FINE). Ultrasound Obstet Gynecol 2013 ; 42 : 268-84. Search the abstract9. Jaudi S, Fries N, Tezenas du Montcel S, Dommergues M. The impact of insonation angle on four-chamber view image quality: an observational study on 2866 routine scans. Prenat Diagn 2015 ; 35 : 382-5. Search the abstract10. Chaoui R. The four-chamber view: four reasons why it seems to fail in screening for cardiac abnormalities and suggestions to improve detection rate. Ultrasound Obstet Gynecol 2003 ; 22 : 3-10. Search the abstract11. Yeo L, Romero R. How to Acquire Cardiac Volumes for Sonographic Examination of the Fetal Heart. J Ultrasound Med 2016 ; 35 : 1043-66. Search the abstract12. Garcia M, Yeo L, Romero R, Haggerty D, Giardina I, Hassan SS, et al. Prospective evaluation of the fetal heart using Fetal Intelligent Navigation Echocardiography (FINE). Ultrasound Obstet Gynecol 2016 ; 47 : 450-9. Search the abstract13. DeVore GR, Medearis AL, Bear MB, Horenstein J, Platt LD. Fetal echocardiography: factors that influence imaging of the fetal heart during the second trimester of pregnancy. J Ultrasound Med 1993 ; 12 : 659-63. Search the abstract14. Tegnander E, Eik-Nes SH. The examiner’s ultrasound experience has a significant impact on the detection rate of congenital heart defects at the second-trimester fetal examination. Ultrasound Obstet Gynecol 2006 ; 28 : 8-14. Search the abstract15. Jaudi S, Granger B, Herpin CN, Fries N, Montcel STD, Dommergues M. Online audit and feedback improve fetal second-trimester four-chamber view images: a randomised controlled trial: Online four-chamber view audit and feedback. Prenat Diagn 2013; 33 : 9 Search the abstract16. Ville Y. “Ceci n’est pas une échographie”: a plea for quality assessment in prenatal ultrasound. Ultrasound Obstet Gynecol 2008 ; 31 : 1-5. Search the abstract