



Fetal imaging
From imaging to clinical diagnosis
Digestive duplications, a case of gastric duplication
Digestive duplications are quite rare, but must be evoked in the fetal ultrasound in front of a rather thick, contiguous, unilocular, regular wall anechogenic image or on the periphery of the digestive tract from the mouth to the anus. Assertion of prenatal diagnosis is difficult, but its possibility makes it necessary to have a meticulous ultrasound balance in search of associated malformative elements and to propose a fetal karyotype. Depending on the situation and the volume of the lesion, possible complications will have to be anticipated in order to prepare for the surgical care of the newborn, or even to organize an in utero transfer if the degree of emergency so requires.
Mrs. T. comes for a first ultrasound at 12 SA and 3 days. The parameters required for the 1st quarter review are normal, the cranial-caudal length (CLA) is 61.4 mm, the nucal clarity is measured at 0.89 mm. There is an additional round image, anechogenic, intra-abdominal, juxta-gastric, similar in volume to the gastric pocket. During the examination, at a prenatal diagnostic meeting, the diagnosis of digestive duplication is discussed. The subsequent ultrasound (18 SA and 3 days, 23 SA and 3 days, 32 SA and 3 days) allows the objectification of a eutrophic fetus, with no other morphological particularity than this intra-abdominal anchogene formation. After a pregnancy of normal evolution, Ms. T. spontaneous delivery at 32 SA and 6 days after spontaneous rupture of membranes without threat of prior delivery and without identifiable etiological factor, of a boy of 1 840 g apgar 8/8/10.
Postnatal support, including tomodensitometry, confirms the diagnosis of isolated gastric duplication. Sturoweight development of the child is normal, but persistent gastro-esophageal reflux leads to the indication of a surgical resection of the duplication, which is performed at 5 months of life by laparoscopy. The suites are simple. The young boy, now 4 years old, has a normal psychomotor and staturoweight development.
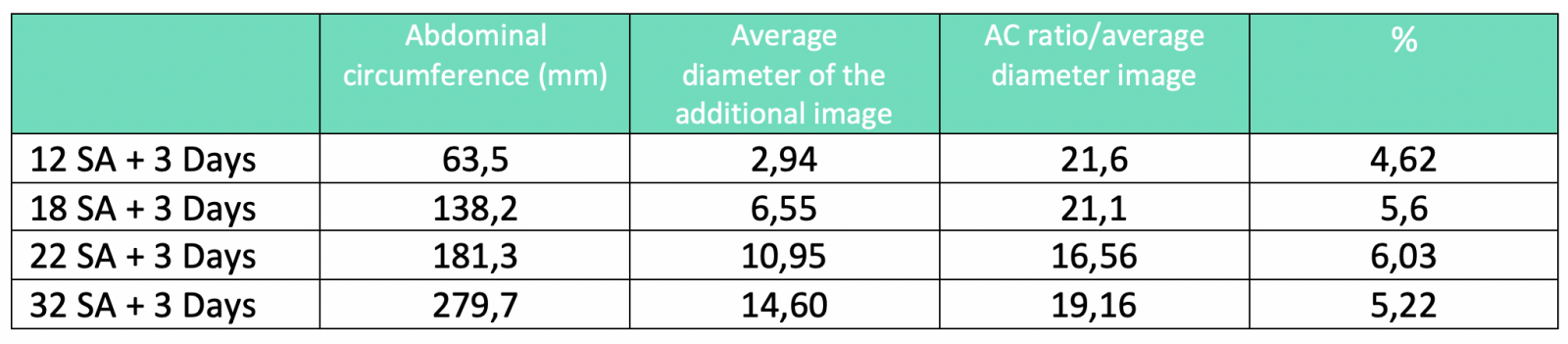
Echographic follow-up suggests that fetal evolution was normal and that this malformation did not affect the fetal growth or vital functions, that the situation, appearance and volume of the stomach were uncharacteristic of the various examinations. The amount of amniotic fluid remained normal from the onset of ultrasound follow-up to delivery. Finally, since we had available the ultrasound parameters of the lesion from 12 to 32 SA, we were interested in the evolution of the dimensions of the lesion in relation to those of the fetus. For this purpose, the ratio of the abdominal circumference to the average diameter of the additional image was made. It should be noted that this ratio is relatively constant from 12 to 32 SA, located around 5% (table). Thus, it appears that the volumetric growth of the lesion has followed fetal growth regularly, without significant acceleration or slowdown.
Rare anomalies
Digestive duplications (DD) are relatively rare birth defects (1/4,000 to 5,000 live births) and represent 0.2 to 0.3% of all malformations). These lesions produce an anechogenic image in ultrasound, with a smooth, thick, regular wall. They may be cystic (90-95% of cases) or more rarely tubular (5-10% of cases). Of varying dimensions, they sit contiguously or on the periphery of the digestive tract from the mouth to the anus. Sometimes communicating with the digestive tract, they are mostly non-communicating (85%) and isolated.
The most frequently found locations are ileal (about 50% of cases), then esophageal (30% of cases), gastric (10%) and colorectal (10%). Oral localization replicas are exceptional but can lead to post-natal emergency surgical management. However, in the latter case, the ultrasound finding of normal in utero deglutition and the absence of hydramnios would be rather favorable prognosis as to the need to intervene urgently to remove the obstacle. Trans-diaphragmatic gastric duplication is possible, which can be switched to second-quarter ultrasound for diaphragmatic hernia. Plural duplications combining thoracic and abdominal localizations are possible.
What complications?
Prenatal complications of DD are mainly represented by ileus and meconite peritonitis. After birth, subocclusive or occlusive symptomatology can be observed by compression, volvulus, or acute intestinal invagination (IIA). The circumstances of SD discovery, sometimes several years in life, may also include abdominal pain, peritonitis by perforation, gastro-esophageal reflux, rectorragy, hematuria, hemoptysis (with blood traces in sputum) for certain thoracic forms and, in very rare cases of communicative duodenal duplication, pancresis acute patient.
Confirmation of diagnosis
Confirmation of the diagnosis of DD is histological with the observation of an external smooth muscle tunic in continuity with the digestive tube musculature and an internal lining suitable for duplication, including at least partially the digestive mucosa. It should be noted that it can coexist within the same lesion of islets of gastric, colic and respiratory mucosa. Pancreatic tissue may also be present in the lesion. The most common aspect of ultrasound is that of a unilocolated spherical cyst measuring 1 to 10 cm in diameter. However, forms of tubular duplications measured up to 85 cm at the anatomopathological examination of the exeresis part are found in the literature. At ultrasound, the wall of the duplication, of the digestive type, has an external hypo-echogenic layer corresponding to the smooth muscle layer and an internal echogenic wall corresponding to the mucosa. The content of the lesion, which is classically anechogenic, can be, much more rarely, ultrasound in case of intracystic bleeding, infection, communication with digestive light.
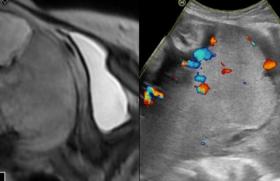
With regard to our observation, at 12 SA, the cutting on the large axis of the embryo, allows to notice an additional anechogenic abdominal image (Figure 1) rounded off from the stomach, a lesion which, on a cross section of the fetal abdomen, produces a smaller image, which seems to "crumble" until the gastric pocket comes into contact (Figure 2). Most often isolated, SD is associated with another malformation in one-third of cases (primarily spinal or lung). Finally, the possibility that a DD will be included in an aneuploidy should lead, if this diagnosis is made, to the realization of a fetal karyotype.

Figure 1 : 12 SA and 3 days.

Figure 2 : 12 SA and 3 days.
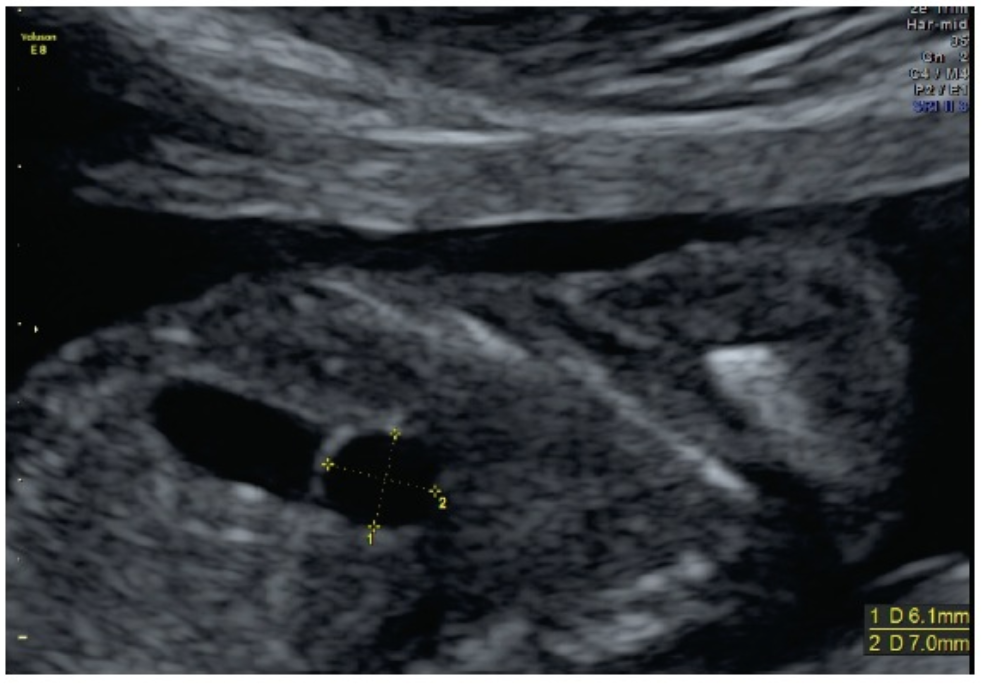
Figure 3 : 18 SA and 3 days.
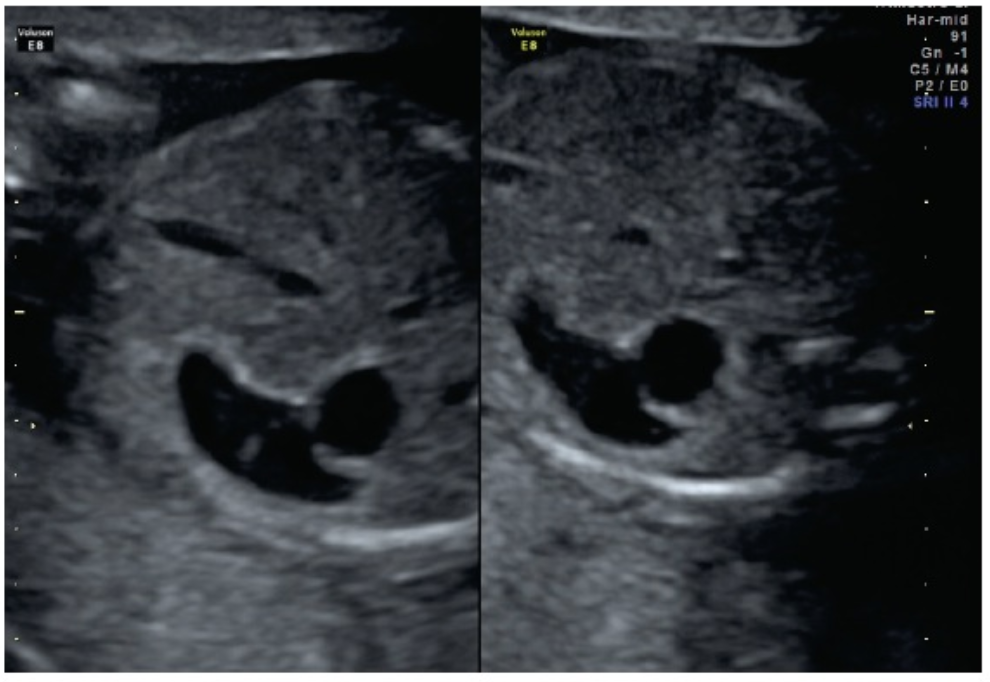
Figure 4 : 18 SA and 3 days.
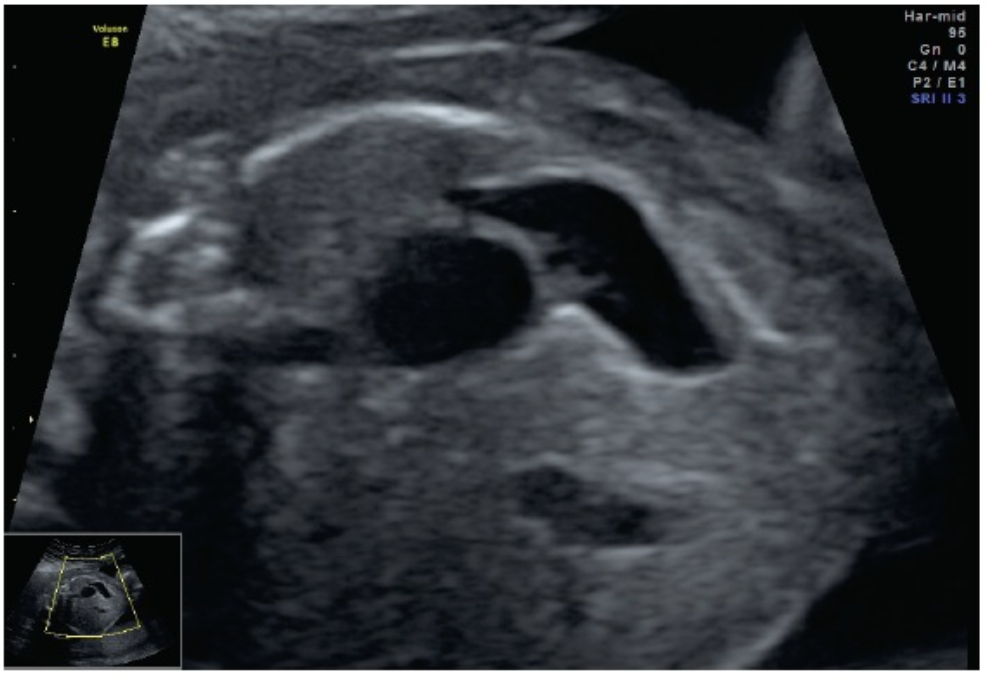
Figure 5 : 22 SA and 3 days.
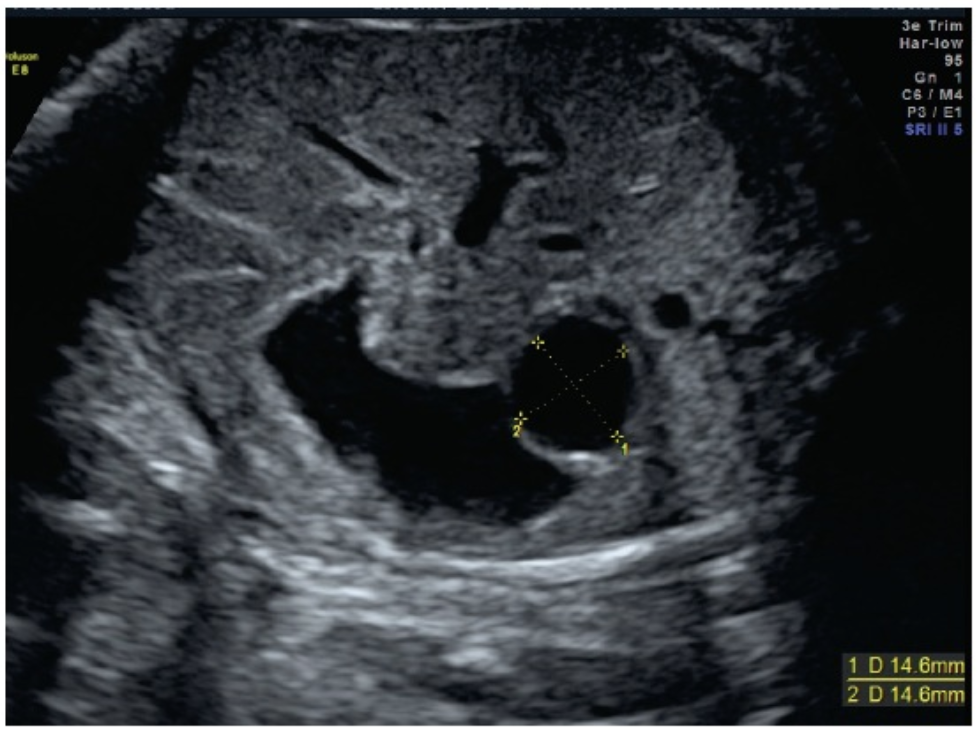
Figure 6 : 32 SA and 3 days.
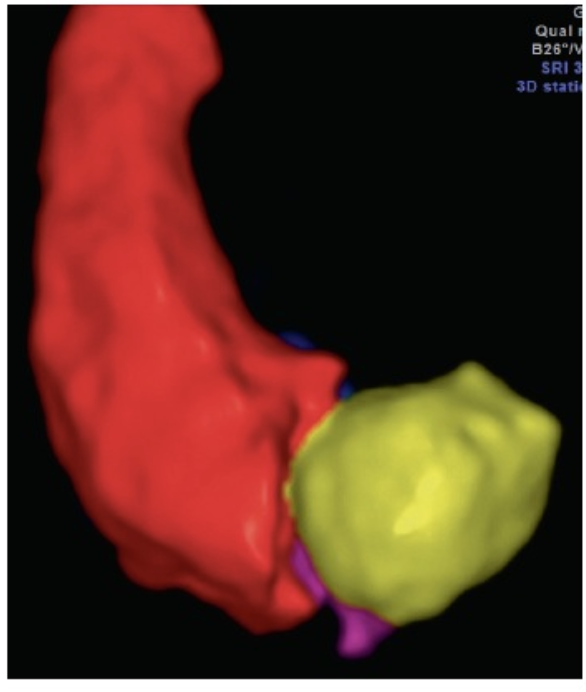
Figure 7 : Gastric volumes and 3D duplication, 32 SA volume reconstruction mode.
Heading coordinated by Jean-Marc LEVAILLANT, Créteil
Articles on the same theme

- 1 of 5
- >
