



Oncology
From imaging to clinical diagnosis
Women at risk of breast cancer - Supervision and management
Screening for women at risk poses two challenges: the risk estimate and the monitoring based on this estimated risk. The modalities of such surveillance should be explained to women so that they can understand the benefits of early diagnosis but also its constraints and limitations (complementary examinations, false positives). It is necessary to educate them to manage their case so that they have all the necessary information and to encourage them to consult if they notice a clinical change. For women with genetic risk, we limit our subject to breast surveillance.
The basic point: appropriate clinical supervision
Clinical examination for possible symptomatology has a fundamental place in breast surveillance. Rigorous, it includes static and dynamic inspection, palpation of the breasts, axillary, subclavicular ganglionic areas and the thoracic wall. The clinical findings are clearly referenced for comparison.
Imaging surveillance capabilities
Surveillance of women at genetic risk
• Monitoring High Risk
Before proposing any surveillance, high genetic risk must be assessed. There are multiple models for calculating risk. The most appropriate approach is to offer the patient an oncogenetics consultation, in order to best assess this risk. Depending on the patient’s results and wishes, the search for a deleterious constitutional mutation will be sought. The value of such consultation is justified on the basis of family history; a simplified calculation is proposed by Eisenger - INSERM-FNCLCC collective expertise(1) (table).
The clinical examination is semi-annual and begins at age 20 for women with BRCA1 or BRCA2 mutations. BRCA1 tumors are undifferentiated and proliferating, interval cancers are more frequent. Imaging surveillance is an option, the alternative being prophylactic mastectomy(2). Despite its mutilating nature, it is the most effective measure to prevent breast cancer risk in a woman with a BRCA1/2 mutation. It is a personal choice that is considered after discussion with the surgeon, the oncogeneticist and consultation with a psychologist.
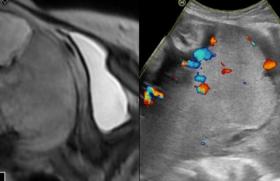
In screening, an annual mammary MRI with dynamic sequences (contrast product injection) is proposed. It is always followed by mammography and ultrasound. This examination allows to search for biopsy-accessible targets if there is an individualized MRI enhancement (Figure 1).
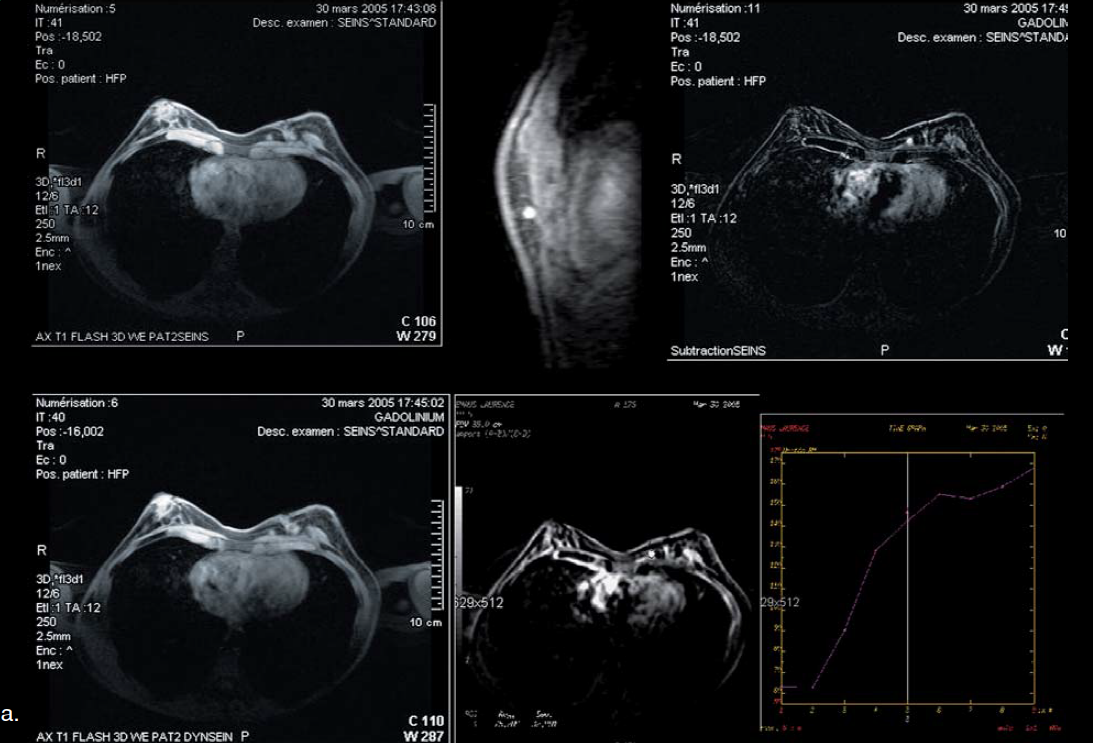
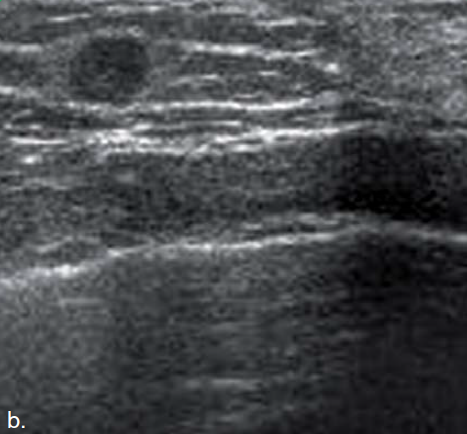
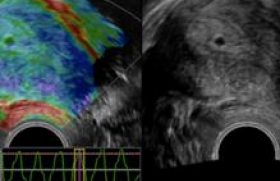
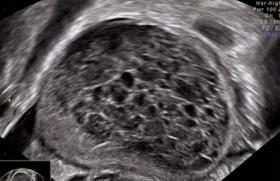
Figure 1 : Personal history of conservative treatment of the left breast (CCI, Grade 3), transferred patient BRCA1. a: Breast MRI: left breast mass (ACR5). Image mammography not seen (very internal anomaly). b: Breast ultrasound (ultrasound microbiopsy), a. histology: KIC.
In France, these recommendations apply to women with a high genetic risk (> 30%). In Europe (EUSOBI) and the United States (American Cancer Society - ACS), this test is prescribed for risks ≥ 20-25%(3). They are defined by the GBA: women with a BRCA1 or BRCA2 mutation, non-mutated 1st degree related patients with a BRCA mutation, women with a cumulative lifetime risk of ≥ 20-25% as defined by family risk factors models(3). It is recommended that imaging be started at age 30(2). Cases justifying earlier radiological monitoring are discussed on a case-by-case basis. The younger, the prevalence of breast cancer and the predictive value are low and must be balanced against the toxicity of X-rays in this population of women who would be more radioactive.
However, mammography should be performed for high-risk patients in order to seek possible calcifications that could be a witness to in situ canalar carcinoma (CCIS). Mammography is numerically preferred for women under 50(4). This surveillance is unlimited.
Before any onset of surveillance, the patient must be informed of the excellent sensitivity of the proposed screening but of the lesser specificity, including MRI, which may induce "false positives" with the completion of additional investigations such as biopsies guided by imaging.
From histological types (the highest frequency of medullary carcinomas for patients) Patients with BRCA1 mutation), the masses of regular contours benefit from microbiopsy because some lesions can result in round shapes with regular contours, evoking adenofibroma, or even cystic lesion (Figure 2).
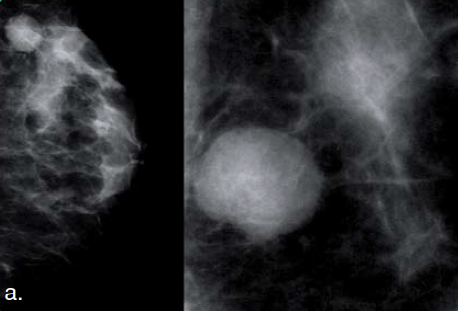

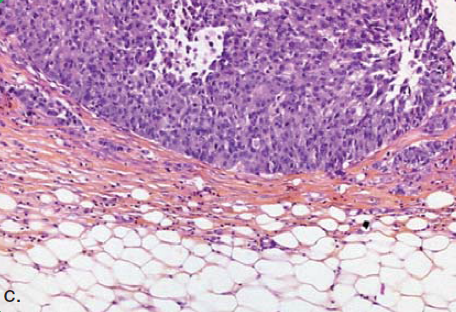
Figure 2 : 32 years old: family history of breast cancer: sister mutated BRCA1. Smooth nodule, moving QSI left breast. a: Mammography, high density round mass with rather narrow outlines. b: Breast ultrasound, hypoechogenic image, homogenous of circumscribed contours with a posterior reinforcement: ACR4a. c: Infiltrating canalar carcinoma, grade 2 RE-, RP+, HER2 -, N-.
• Surveillance of Moderate-Risk Women
The most difficult assessment of this risk is; however, this estimate will depend on the type and rate of surveillance. Consultation of oncogenetics may be proposed using the same criteria as previously. Generally, mammography is annual (digital for women < 50 years of age) associated with ultrasound. If the lifetime risk is less than 15-20%, there is no indication for or against the completion of a breast MRI, decisions are made on a case-by-case basis (ACS). On the other hand, a consensus of expert opinion does not recommend a screening MRI if the cumulative lifetime risk is less than 15%(3).
Surveillance of women with personal histological risk
• Breast Surveillance
Within this framework, the relative risk of recurrence or discovery of another cancer is increased. All available texts confirm the Cochrane synthesis article (2000): surveillance is based on the biannual clinical examination for 5 years, then annual, and mammography ± annual ultrasound without limitation. No other monitoring modality has been shown to be of benefit to patients with BRCA1/2 mutation who are treated for non-metastatic localized breast cancer. The natural history of breast cancer shows that after the 2- and 5-year repeat spikes, "events" continue to appear regularly at a rate of 1-2% per year, in a way that is consistent with the current pattern of the occurrence of breast cancer cumulative and without a time limit. The risk of controlateral breast cancer is 2.5 times higher than in the general population.
- The recommendations call for annual mammographic surveillance without limitation of duration(5). After a conservative treatment, a mammogram is performed 6 months after the end of the radiotherapy for a post-therapeutic reference examination (Figure 3).
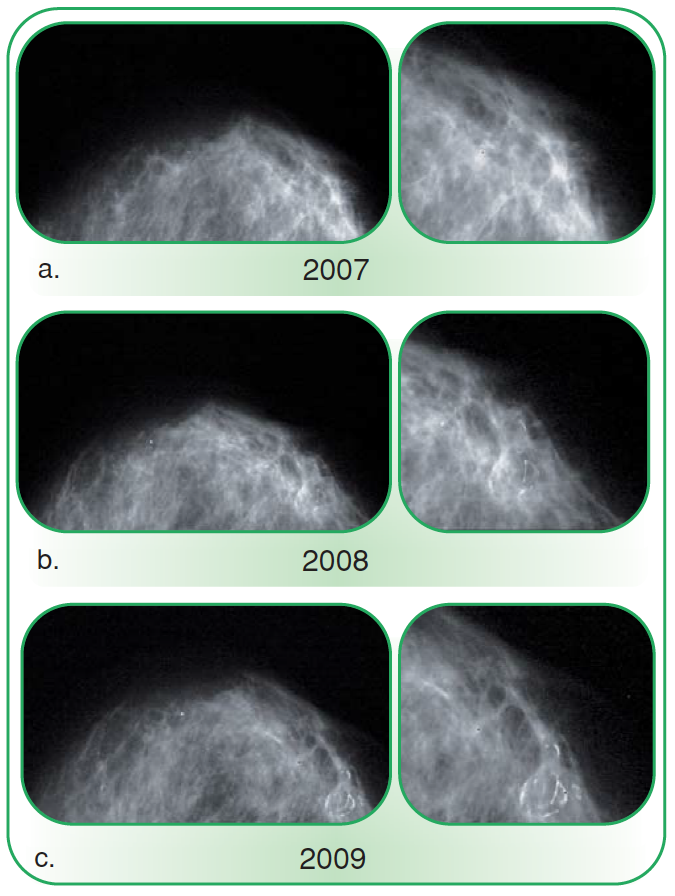
Figure 3 : 64 years old: history of conservative right breast treatment (2006). Nodule at the scar. a: Post-therapy photograph (6 months after the end of radiation therapy): clearly limited image (next to the palpated nodule): cytosteatonecrosis - ACR2 (benign findings). b: Clear image with peripheral calcifications: calcified cytosteatonecrosis - ACR2. c: "Hard" nodule: Clear image with peripheral calcifications next to it: cytosteatonecrosis whose calcifications complement each other - ACR2.
Two shots per breast are made. Analog mammography and digital mammography have comparable efficacy(4). However, in sub-groups of women under 50, in perimenopause or premenopause, or with dense breasts (types 3 and 4 density according to BI-RADS), digital mammography is more effective. The advantage of digital mammography is undeniable for image transmission and storage (PACS). It is important to have the entire file, including the clichés before and immediately after the intervention.
- The association with an ultrasound is carried out during a difficult analysis or in dense breasts. It allows the study of axillary ganglionic areas and the thoracic wall. A study of 2,725 high-risk women (1,443 of whom had breast cancer) showed that ultrasound increased the sensitivity of cancer detection, but increased the risk of false positive(6). The cancers detected by ultrasound in this cohort are small infiltrative cancers without ganglionic impairment.
There is no evidence in the literature to recommend a surveillance MRI on a systematic basis. This examination is offered to patients where there is a diagnostic doubt (scar versus recurrence). MRI has a sensitivity that is greater than 90%. The specificity of MRI is also high and above 90%. If the lesion is not accessible or not seen in ultrasound, the sampling will be guided under MRI. The sensitivity of the MRI is significantly lower in CIHIs (two-thirds of cases in the same form). Subgroups of women should benefit from this review when there are genetic risks associated with : BRCA1/2 mutation, untested 1degree related patient with BRCA mutation, cumulative risk over life of more than 20-25%. These indications are consistent with the GBA(3) recommendations. The other indications for the realization of breast MRI are to be discussed "on a case-by-case basis" at multidisciplinary consultation meetings (PCRs): when initial cancer is not detected by mammography, in young women (under 35/40 years), in dense breasts, triple negative patient. The impact on mortality is not yet known.
• Lamb surveillance after breast reconstruction
A literature review shows that the arguments are weak to propose a systematic mammography of the lamb. No recommendations are proposed.
• Monitoring of the prosthesis after mastectomy reconstruction
If there is a suspicion of rupture, this surveillance is comparable to the exploration carried out during the installation of prosthesis with aesthetic purpose (digitized costal profile, ultrasound, MRI). Note the importance of clinical review: prosthesis and search for repeat or permeation nodule.
• Surveillance after histological diagnosis of atypical epithelial hyperplasia (HEA), in situ lobular carcinoma (CLIS)
As the risk is increased, mammographic surveillance is identical to that of treated breasts. Mammography will be annual without limitation. Breast ultrasound is performed in the same way.
Surveillance of dense breasts
Breast density is a significant and independent factor of breast cancer, generalizable to different populations. High density suggests that this parameter should be considered for inclusion in predictive factors for breast cancer. Based on the published data, digital mammography should be preferred in dense breasts in women under the age of 50. Dense breasts are responsible for a higher rate of cancer in the interval than fat breasts. Between the ages of 40 and 49, an annual mammogram or every 18 months is recommended. Follow-up will then be biennial, as part of organized screening (DO). An ultrasound is justified; This review must be comprehensive and rigorous, with strict diagnostic criteria for malignancy to avoid high follow-up rates or interventional gestures for benign lesions (false positives).
Currently, no Phase III study has assessed the value of MRI in dense breasts screening. While MRI is a very sensitive examination, its impact remains unknown in this context. The problem remains the evaluation of breast density, which is difficult to reproduce. Assessment is qualitative in routine, but there are no standardized methods of quantification. As a result, this data is not included in predictive models of breast cancer risk.
Surveillance of women with hormonal treatment of menopause (THM)
There is no need to propose surveillance in particular imaging, mammography is biennial, as part of organized breast cancer screening between the ages of 50 and 74. If the breasts are dense, nodular, difficult to analyze, an ultrasound will complete this assessment.
Surveillance of women with chest irradiation
Thoracic radiation increases the risk of breast cancer, especially when irradiation is performed before 30 years. Mammographic surveillance is annual and supplemented by ultrasound. Although there are few published studies of MRI performance in this indication, the GBA recommends annual MRI for patients with chest irradiation between the ages of 10 and 30(3).
In practice
• For women with a family history of breast or ovarian cancer
Risk assessment is required : an oncogenetics consultation is appropriate in cases determined by the INSERM-FNCLCC collective expertise (table above).
The clinical examination is biannual.
- In the context of high risks: a mammary MRI is performed followed by a mammogram, associated with a mammary ultrasound. These reviews are conducted over 30 years.
- In the context of moderate risks: follow-up is comparable, except for MRI, which is not indicated if the risk is < 15-20%. Women who had a chest irradiation before 30 years of age (Hodgkin's disease) are considered to be at a risk comparable to women who had a BRCA1 mutation. The follow-up will therefore be identical.
• For women with a personal history of risky cancers or histological lesions
The clinical examination is biannual for 5 years (breast cancer CD) and annual. A mammogram ± an annual ultrasound with no time limitation is recommended. The MRI has specific indications and needs to be discussed in PRR. There is no indication that a lamb-reconstructed breast mammogram will be performed.
• For women with dense breasts
Between 40 and 49 years, the tighter rate of surveillance is recommended (12 or 18 months). After 50 years, women have a mammogram every 2 years, as part of organized breast cancer screening (DO). Breast ultrasound is always performed.
Points to determine |
Women at genetic risk
|
References
Click on the references and access the Abstracts on

1. Eisinger F, Bressac B, Castaigne D et al. Bull Cancer 2004 ; 91 : 219-37. Search the abstract2. Institut National du Cancer (INCa). Principales recommandations de prise en charge des femmes porteuses d’une mutation de BRCA1 ou BRCA2 (2009). www.e-cancer.fr Search the abstract3. Saslow D, Boetes C, Burke W et al. CA Cancer J Clin 2007 ; 57 : 75-89. Search the abstract4. Pisano ED, Hendrick RE, Yaffe MJ et al. (DMIST Investigators Group). Radiology 2008 ; 246 : 376-83. Search the abstract5. Aymard L, Barreau B, Burnel S et al. Principes et modalités de la surveillance des cancers du sein. 11e cours Francophone Supérieur sur le cancer du sein de Nice-Saint Paul (14-17 janvier 2009). Search the abstract6. Berg WA, Blume JD, Cormack JB et al. JAMA 2008 ; 18 : 2151-63. Search the abstract
Articles on the same theme

- 1 of 5
- >
