



Obstetric imaging
Placental MRI
The placenta is a complex organ that is essential for fetal growth and development. He is involved in the fœtal-maternal exchanges as early as the fifth week of amenorrhea. The human placenta is said to be of a hemochorial type, i.e., the choral villi are in contact with the maternal blood, unlike the epitheliochorial placenta (as in ruminants), or the endotheliochorial placenta. Proper infusion and permeability of the place are essential.
Placental insufficiency, as well as placental invasion abnormalities, are major public health problems with high fetal and maternal morbidity and mortality. In fact, placental insufficiency is the leading cause of fetal/neonatal morbidity and mortality, and the placenta accreta, or even percreta, has a high maternal morbidity with complex management.
The exploration of the placenta in imaging is currently based on ultrasound, whose objectives are to define its location or to detect implantation anomalies (placenta praevia, placenta accreta). One of the major areas of research to better understand placenta abnormalities in vivo is imaging, and in particular MRI, which is used to evaluate the function and invasion of placenta. Several studies have confirmed the safety of MRI in pregnant women. The sequences used are made to minimize the specific absorption rate (DAS), with adapted view fields.
The normal placenta has an intermediate T2 signal, more hyposignal than the myometer. Dissemination sequences (DAS: 0.1 watts/kg) can be used. Finally, placental vascularization remains a major focus, still unknown. Due to the precautionary principle, gadolinium injection remains confidential due to the lack of data in the human fetus. However, recent studies have suggested a certain interest in injected sequences to increase the contrast between placenta and myometer, useful for the analysis of placental insertion anomalies. In practice, gadolinium injection may therefore be useful in certain situations, but will have to be done as close as possible to the date of issue, in agreement with the obstetric team, to avoid the prolonged stagnation of the contrast product in amniotic fluid (Figure 1).
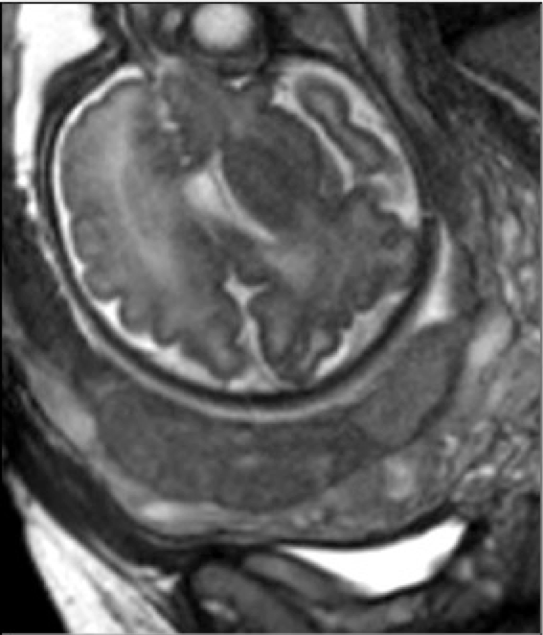
Figure 1: Example of T2 HASTE sequence placenta MRI: the placenta is more hyposignal than the myometer. The retro-placental edge is perfectly followed in the form of a T2 hyposignal end.
Placental insufficiency
It corresponds to placental dysfunction, which is most often linked to an infusion defect resulting in a decrease in the supply of oxygen and nutrients to the fetus. It is responsible for frequent, potentially severe maternal-fetal diseases, the two main of which are pre-eclampsia and intrauterine growth retardation (IUCN).
Several MRI techniques are now used to understand in vivo the functioning of the placenta.
• MRI with contrast product injection (DCE-MRI)
This is the historic technique for measuring organ infusion. Image acquisition will take place before, during and after the injection of a contrast product. The kinetics of enhancement of the organ of interest will be analyzed in comparison with the increase obtained in the arterial vascular sector (cardiac cavity and/or large vessels).
The functional parameters are obtained from the pharmacokinetic modeling of the contrast agent distribution. Depending on the models used, several functional parameters can be obtained: blood flow, infusion, blood density, surface permeability coefficient.. These parameters can also be used to generate color-coded images that assist in the visual evaluation of tissues (parametric map).
Only animal studies are available in the literature. Our team has developed several approaches to study placenta in mice or rats using a contrast agent. We have mainly used commercially available Gd chelate (Dotarem®), which crosses the maternal-fetal barrier in the placenta.
DCE-MRI is likely to remain the most robust way to evaluate the in vivo placental function to date. It allows direct quantification of blood flow and is based on a well-standardized methodology that has been fully described. On the other hand, the use of contrast products in pregnant women remains highly discussed and these techniques cannot be transposed into clinical settings at the moment (Figures 2a and b).
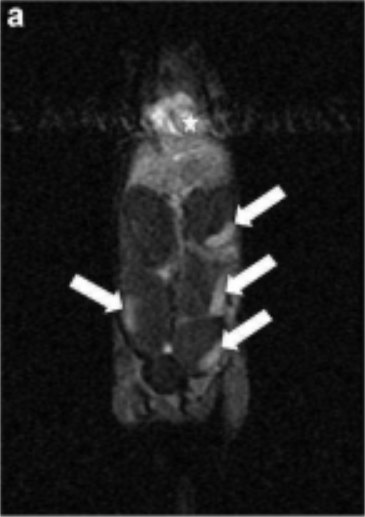
Figure 2a: Example of a dynamic sequence after injecting gadolinium into the mouse. In this coronal image, four placentas are shown with a post-injection enhancement (arrows). The left ventricle increases early and intensively, with a peak, which corresponds to the first passage. The elevation observed in the placentas is less intense and more progressive. Note that there is no fetal enhancement.
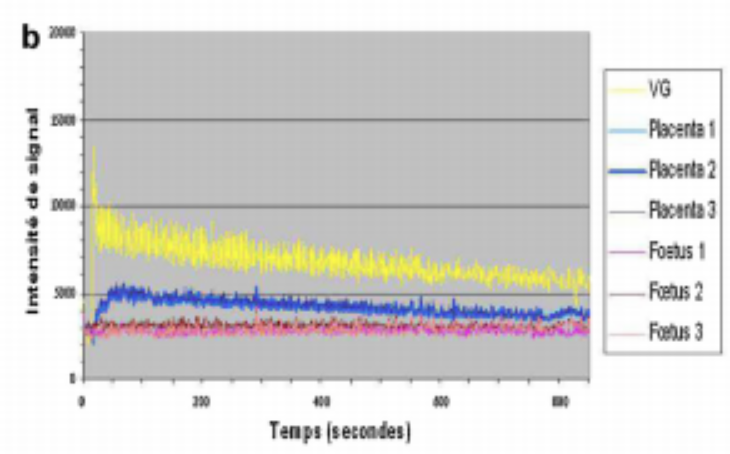
Figure 2b: Example of a dynamic sequence after injecting gadolinium into the mouse. Example of signal strength curves (IS) for the left ventricle (VG) and three placentas and fetus after gadolinium injection. The left ventricle increases early and intensively, with a peak, which corresponds to the first passage. The elevation observed in the placentas is less intense and more progressive. Note that there is no fetal enhancement.
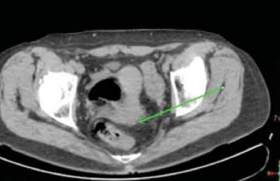
To evaluate the use of DCE magnetic resonance imaging during pregnancy, placental transfer data and normal placental infusion ranges should now be established. A research protocol, PLACENTIMAGE, to evaluate the feasibility of MRI DCE in pregnant women and to build reference standards for placental infusion has been completed (Figure 3).
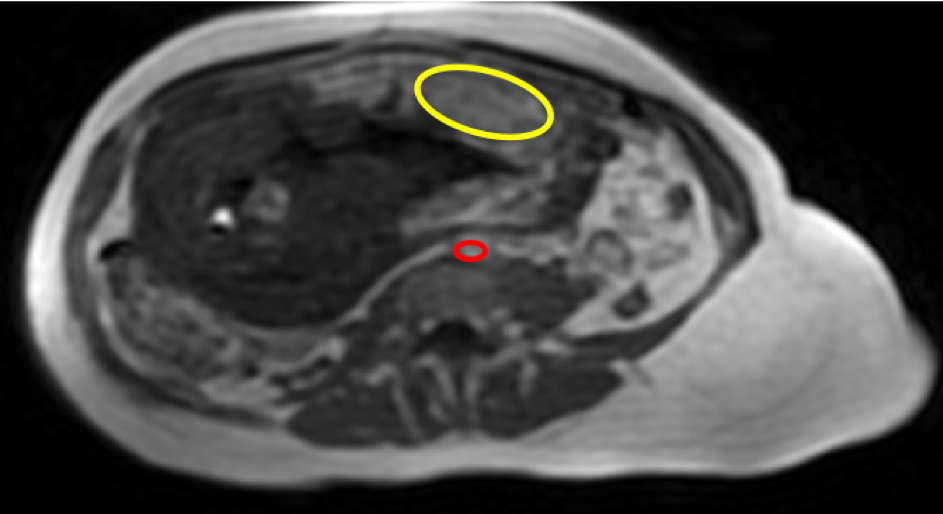
Figure 3: Example of a dynamic sequence after injection of gadolinium into humans. On this axial image, a region of interest is positioned on the placenta (yellow) and aorta (red).
• BOLD MRI
This technique uses hemoglobin (Hb) as an "endogenous contrast agent" to visualize a function rather than a structure. Deoxyhemoglobin (dHb) has paramagnetic properties and induced a decrease in T2 and T2*. In contrast, oxyhemoglobin has diamagnetic properties. The BOLD effect therefore measures the difference in signal and or T2* between two different oxygenation states: a reference (normal or resting state) and a hypo/hyper-oxygenation status (or active state).
Changes in hemoglobin oxygen saturation in capillaries can be detected by changes in SI or by changes in T The first BOLD MRI-based publications
during pregnancy were experimental on animal models. The MRI BOLD is also able to detect an abnormality in placental functioning in the context of intrauterine growth retardation. Indeed, several studies in animals, but also in humans, have shown that placentas do not have the same BOLD effect in CIDR. situations. This technique could thus allow the early detection of dysfunctional placentas.
MRI BOLD could also be used for functional imaging of the fetal brain. Some technical difficulties, however, need to be overcome. A BOLD MRI clinical trial in pregnant women as a non-invasive diagnostic tool for placental failure is currently underway.
• Arterial Spin Labeling (ASL)
IRML MRI ASL is another MRI technique that can be used to evaluate placental infusion. Intravenous injection of contrast product is not required. The MRI ASL uses the magnetization of blood entering the organ of interest. Water in blood is used as an endogenous tracer. This water is marked in an area of interest by a selective radiofrequency (RF) pulse that reverses the signal of the blood protons. Two acquisition sequences are needed.
The subtraction of marked and unmarked images "in pairs" gives a signal difference that reflects tissue infusion, since the signal difference is related to the arterial protons marked in motion (Figure 4a and b).
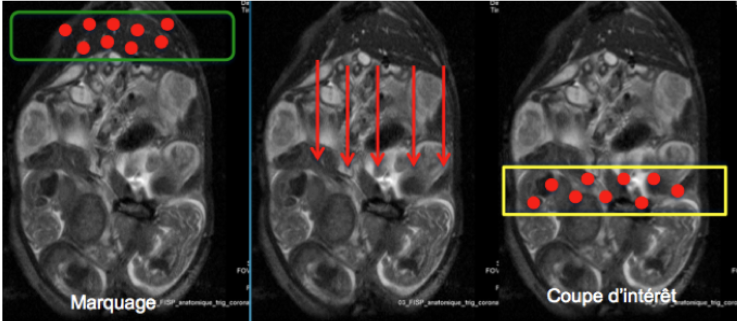
Figure 4a: The ASL principle illustrated in the pregnant spleen: the anatomical reference image is a coronal image of pregnant spleen in which foeto-placental units are visualized. The figure shows the production of the tagged image. In the most left image, the tag is performed by magnetic inversion outside the study area (green box) and leads to spins marked in the blood (red dots). A delay before the acquisition is necessary for the progress of the marked spins towards the area of interest: transit time (image of the middle). Next, the acquisition is made at the (yellow) level of interest containing the spins marked (right image).
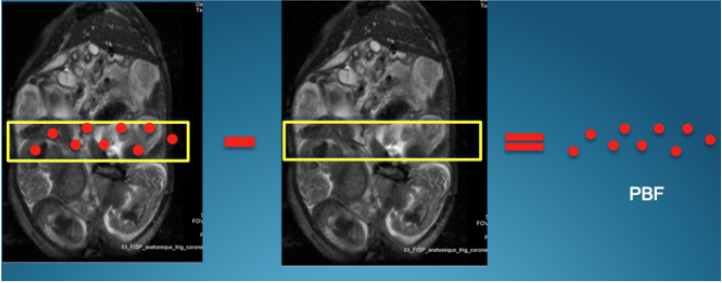
Figure 4b: The ASL principle illustrated in the pregnant spleen: the anatomical reference image is a coronal image of pregnant spleen in which foeto-placental units are visualized. Images called "tagged" and "controls" are then "subtracted" to preserve only the signal of the mobile protons contributing to tissue infusion. The residual signal thus reflects the infusion, here the placental blood flow (PBF).
Some studies have been carried out in the animal and the very promising technique is beginning to be tested in the human placenta. The current applications of ASL in humans are mainly related to cerebral infusion (Figure 5).
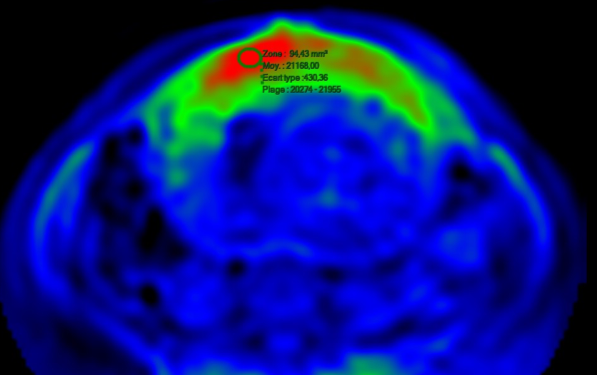
Figure 5: An example of placental flux mapping obtained by ASL in humans.
• Intra Voxel Incoherent Motion (IVIM) and scattering MRI
Dissemination imaging provides a contrast by measuring the movement of water molecules in tissues, which decreases the signal.
The IVIM concept (Intra Voxel Incoherent Motion) is based on the assumption that the weighted signal in scattering in a voxel depends on two compartments. The first compartment is composed of extravascular water molecules (thermal Brownian movement), whose displacement corresponds to diffusion. The second compartment is composed of intravascular water molecules circulating in the hair network, the displacement of which corresponds to an infusion (or pseudo-diffusion). The apparent diffusion coefficients (ADCs) and the IVIM parameters are obtained from the signal decay curve at different b.
The IVIM parameters are calculated from a bi-exponential decay of the signal intensity curve based on the b values. Three parameters are obtained: the diffusion coefficient (D, 10-3 mm2/s) that reflects tissue diffusion while the other two — the perfusion fraction (f, %) and pseudo diffusion coefficient (D*, 10-3 mm2/s) — are related to microcirculation. For placenta imaging, f is likely to represent the fraction of blood volume moving relative to the total volume of voxels. D* would reflect the circulation of blood in intercity spaces and in capillaries within fetal villi. D reflects the cellular and pore characteristics of the tissue.
Several studies have established the values of the main parameters in the animal. In humans, several studies have also suggested that the parameters of IVIM and placental diffusion would be disrupted in the event of delayed intrauterine growth.
Measuring ADC may be useful for detecting structural changes in the IUGR placenta. Analyzing IVIM with a more accurate measurement of the f infusion fraction may be interesting for diagnosis of placental failure in IUGR and preeclampsia, a non-contrast technique for the evaluation of infusion.
Placental insertion abnormalities
• Placenta praevia
This corresponds to a low insertion of the placenta on the lower segment of the uterus within 2 cm of the inner hole. It can be partially or completely covered on the collar. Low placental location is common at the beginning of pregnancy (25%) before 20 SA. With the development of the lower segment, the percentage is reduced to 1% in the 2nd and 3rd quarters. Its prevalence increases with maternal age and number of cesarean sections.
Abdominal ultrasound is usually sufficient for diagnosis of placenta praevia with a sensitivity of 93-97%. MRI has little added value for this diagnosis, except for posterior placental location (Figure 6).
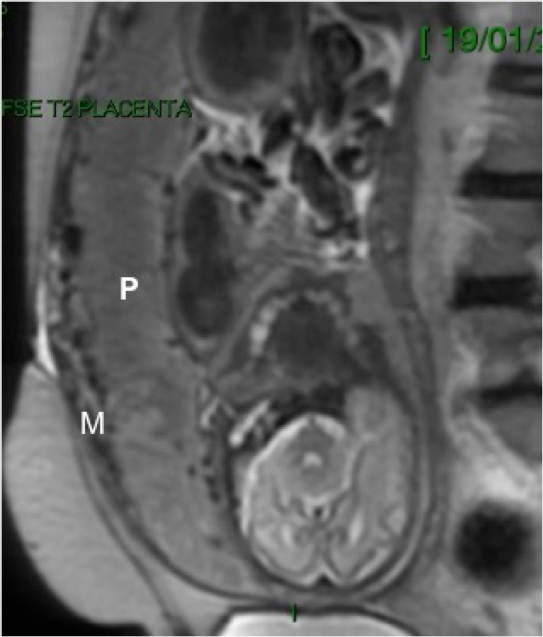
Figure 6: Example of placenta praevia (P) in HASTE T2 sagittal sequence; Note that the myometer (M) is particularly thin at the lower segment.
• Placenta accreta (invasive abnormal placenta)
The placenta accreta is clinically defined by abnormal adhesion of the placenta to the uterine wall resulting in no cleavage during delivery. This pathology is secondary to an abnormal invasion of chorial villi within the myometer. Three types of "placenta accreta" are distinguished by the depth of myometrial invasion (i.e. accreta, increta, percreta). The placenta accreta is the most common type (60-78%), with villi penetrating superficially within the myometer without depth extension. In the placenta increta (20%), the villi invade the entire thickness of the myometer without crossing the serous. The placenta percreta (5-20%) represents the most severe form, where placental tissue invades the entire myometer with extension beyond the serum and possibility of extension to adjacent organs.
MRI is currently performed almost systematically when there is clinical and ultrasonic suspicion of placenta accreta.
Several diagnostic criteria T2-weighted MRIs were proposed to suggest diagnosis: heterogeneous or "bombant" appearance of the placenta on the uterine serum, dark bands in "hyposignal T2" perpendicular to the myometer-placenta interface, interruption of the retro-placental edge with exophytic placenta within the myometer, placental tissue extension beyond the uterine serum to adjacent organs. Despite the lack of consensus on the use of gadolinium during pregnancy, its potential interest in injected sequences relative to T2 sequences, for a better tissue contrast between myometer and placenta after 30 SA, may be interesting. Since the toxicity of gadolinium remains unknown on the fetus, the European Radiology Society reserves its use in cases where the diagnostic benefit is significantly greater than the risks to the mother (Figures 7a, b and Figure 8).
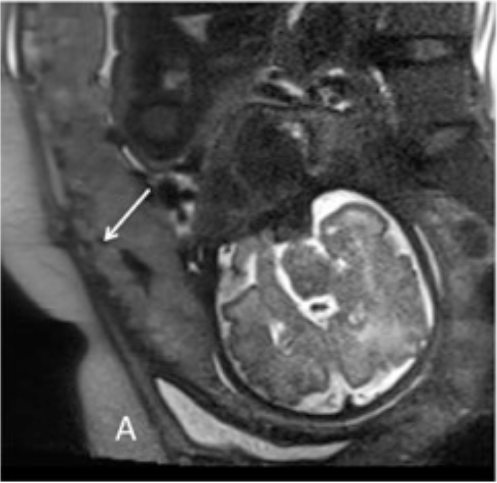
Figure 7a: Example of a suspicious placenta on the classic HASTE T2 sequence.
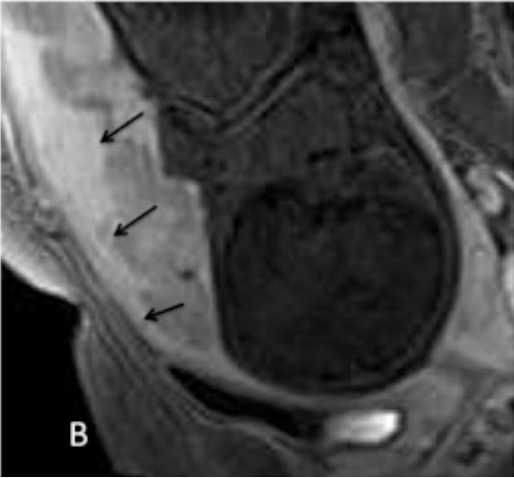
Figure 7b: Example of a suspicious placenta of accreta on the classical HASTE T2 sequence reversed by the sagittal T1 sequence with gadolinium injection where the placenta-myometer interface is well distinguished.
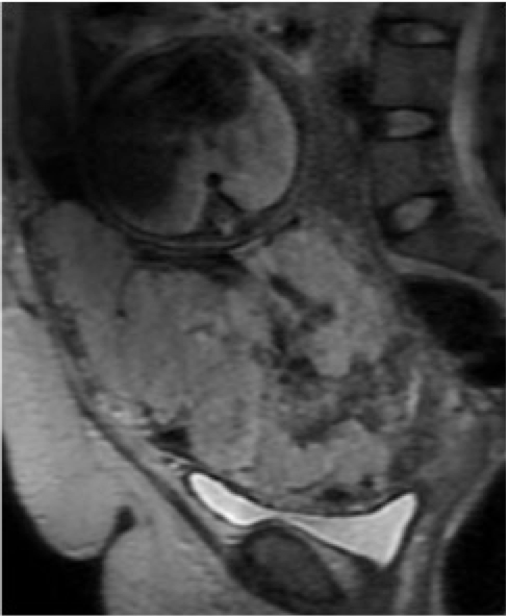
Figure 8: Example of placenta percreta in a sagittal sequence Haste T2: the placenta is bulky, heterogeneous, with several dark bands perpendicular to the backward edge. No healthy myometer can be distinguished between the bladder and the placenta, which invades the bladder.
• Cord placental insertion abnormalities: vasa praevia
Screening for praevias vasa is crucial because it is particularly dangerous, due to the risk of Benckiser’s procidence or bleeding when a praevia vessel breaks up at membrane opening. These are low or velvety marginal insertions (1/500), This anomaly often results from asymmetrical placental resorption on an initially inserted low placenta. It is primarily screened in ultrasound, but MRI can be useful to confirm the venomous insertion and exact topography of the placenta.
Conclusion
The MRI is therefore complementary to ultrasound and well adapted for the diagnosis of placental insertion anomalies, particularly in the assessment of the depth of invasions type percreta. In addition, early identification of high-risk fetuses of IUCN is one of the challenges in modern obstetrics. The placenta functional MRI represents an interesting imaging perspective for tracking high-risk pregnancies. However, despite the availability of many MRI techniques to study the functioning of the placenta, in vivo studies of the human placenta are still rare. The respective interests of each method should be quickly understood and a standardization of techniques is necessary to enable obstetric MRI to find the place it deserves !
Articles on the same theme
- <
- 2 of 2